For you. For your birth. For your baby. Be informed.
Standards of Care in Newborn Delivery
Standards of Care are the guidelines set forth by a healthcare profession (such as doctors or midwives) that help those professionals and the public stay informed about what quality health care looks like, based on current evidence and common practice. Standards of Care also help us identify care (or lack-of-care) that is NOT acceptable based on available research. In the event of a malpractice case, a health professional will be held to account based on that profession’s standards of care.
These organizations develop bulletins or statements to keep the members of their field informed of important evidence and consistent in their practice. As of this writing, ACOG has issued nearly 200 Practice Bulletins on preventive care, surgical, and labor and delivery topics for their members. The AAFP has issued Clinical Practice Guidelines on the broad range of topics in family medicine from ear infections, to obesity, to Vaginal Birth After Cesarean. Likewise, the ACNM has issued a number of Position Statements across various women’s health topics, including labor and delivery.
…each midwife is an individual with specific practice protocols that reflect her own style and philosophy, level of experience, and legal status, and that practice guidelines may vary with each midwife. NARM does not set protocols for all CPMs to follow, but requires that they develop their own practice guidelines in written form.
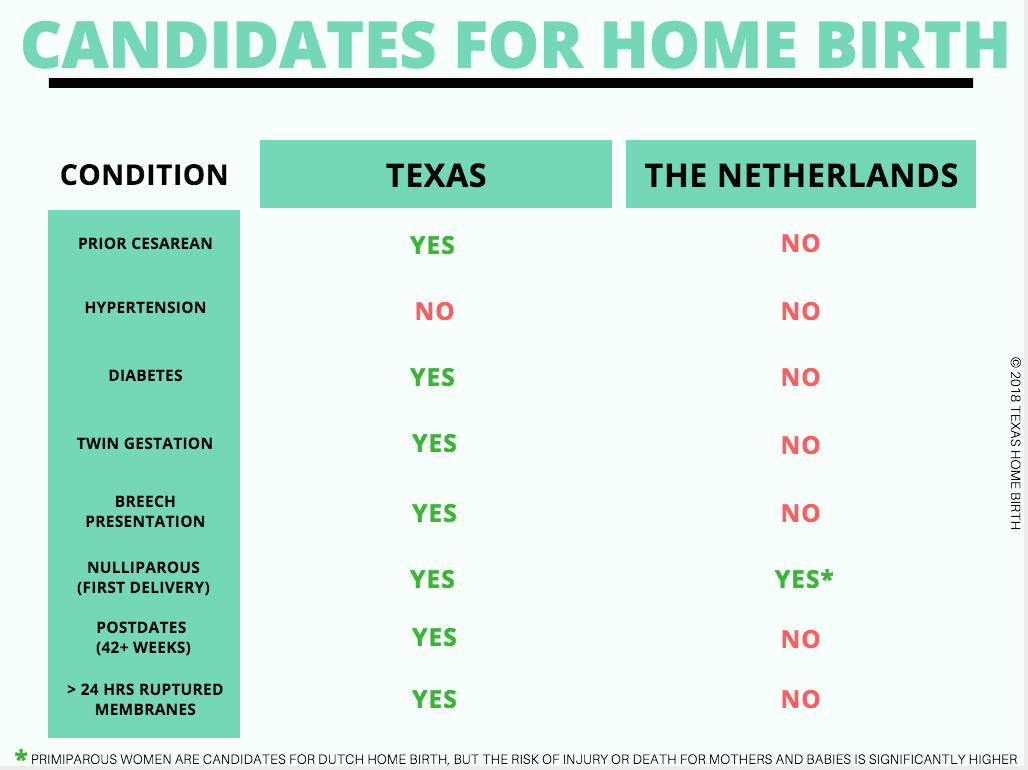
This means that a CPM in America can choose to deliver the babies of high-risk women who would not meet criteria for home birth in other countries. The non-nurse midwife may also choose to deliver babies in breech presentation, or babies with other factors that have been shown to increase risk of death. Other CPMs might be well aware of these risks and have strict criteria for the clients they accept for home or birth center birth. However, this lack of standard practice across CPMs may contribute to poor outcomes for mothers and for babies in America. You can read more on the EVIDENCE page. The infographic below helps explain the differences in risk criteria between home birth in the US versus in The Netherlands, where home birth is generally as safe as hospital birth for both mothers and babies.
A lack of written standards also makes it hard to hold a midwife accountable for bad decision-making or poor risk management. NARM suggests a peer review process for member CPMs, but this is completely voluntary and happens at the local level through regional midwife organizations. Peer review for physicians and nurses in hospitals is not voluntary, as hospitals must conduct peer review to keep their accreditation. More information about accountability for different birth attendants is available on the REGULATION page.
There is a mechanism for grievances and complaints that could lead to loss of a midwife’s CPM credential. Prospective clients should note that a midwife can have her CPM revoked and still continue to practice in her state, if her state does not require the credential for practice (such as in Texas). NARM has revoked the credential of a total of six midwives in the 26-year history of the organization. State accountability procedures are discussed on the REGULATION page.
Rules Specific to Texas
While there are no national guidelines from NARM to standardize the practice of midwifery, The Midwives Program at the Texas Department of Licensing and Regulation has established a Standards of Care Workgroup specific to Texas direct-entry midwives. The workgroup has developed administrative rules to guide the practice of midwives in the state. Remember, these rules only apply to Texas Licensed (non-nurse) Midwives.
It’s important for every client to know what a home birth midwife is and is not allowed to do for her in the prenatal period, at a Texas home birth, or postpartum. Relevant portions of the administrative rules are provided here with some edits for clarity and readability only.
Prenatal Care
If your midwife discovers you have any of the following, she must recommend referral to a physician or delegate of a physician (perhaps a certified nurse midwife, the rules do not explain who this associate could be).
infection requiring antimicrobial therapy;
Hepatitis;
non-insulin dependent diabetes;
thyroid disease;
current drug or alcohol abuse;
asthma;
abnormal pap smear (consistent with malignancy or pre-malignancy) during the current pregnancy;
seizure disorder;
prior cesarean section (except for prior classical or vertical incision, which will require transfer in accordance with subsection (c)(8));
multiple gestation;
history of prior antepartum (miscarriage) or neonatal death;
history of prior infant with a genetic disorder;
significant vaginal bleeding;
maternal age less than 15 at Estimated Date of Conception;
cancer or history of cancer;
psychiatric illness; or
any other condition or symptom which could adversely affect the mother or fetus, as assessed by a midwife exercising reasonable skill and knowledge
This referral means that you and your physician (or their associate/CNM/PA, etc) will together determine whether you and your baby are still good candidates for home birth. Your care from this point forward may be with:
Your midwife alone
Collaboration between your midwife and physician
Only with your physician, if your condition requires expert management
As the client, you have the right to refuse this referral or to not accept the physician’s advice, and your midwife must document your choice in your record. She may legally continue to care for you if you refuse referral so long as she seeks a consultation with a physician(doctor) or collaborates with an appropriate health care professional which must be either a physician or another clinician working under supervision of a physician. She can then co-manage your care with this provider or terminate your midwife-client relationship..
Sometimes a condition is so dangerous to you or your baby that a simple referral for a doctor’s advice is not enough, and transfer of care is required. Transfer means that a midwife relinquishes care of the client for pregnancy, labor, delivery, or postpartum care or care of the newborn to another health care professional who has current obstetric or pediatric knowledge and is either a physician licensed in the United States; or working in association with a licensed physician. To better understand the risks of different conditions for yourself as they relate to home birth, please review the EVIDENCE page. The following conditions require transfer of care:
placenta previa in the third trimester;
Human Immunodeficiency Virus (HIV) positive or Acquired Immunodeficiency Syndrome (AIDS);
cardio vascular disease, including hypertension, with the exception of varicosities;
severe psychiatric illness;
history of cervical incompetence with surgical therapy;
pre-term labor (less than 37 weeks);
Rh or other blood group isoimmunization;
previous uterine surgery involving incision into the uterine myometrium, other than a low transverse cesarean section
preeclampsia/eclampsia;
documented oligo-hydramnios or poly-hydramnios;
any known fetal malformation;
Preterm Premature Rupture Of Membranes (PPROM);
intrauterine growth restriction
insulin dependent diabetes;
triplet or higher order multiple gestation;
active cancer history or history of ovarian, breast, uterine, or cervical cancer;
undiagnosed vaginal bleeding lasting longer than two weeks, or;
any other condition or symptom which could threaten the life of the mother or fetus, as assessed by a midwife exercising reasonable skill and knowledge
If a client has reached 42 weeks, zero days gestation and is not yet in labor, the midwife must immediately either:
collaborate with a physician and obtain appropriate antenatal testing, in order to continue midwifery care; or
initiate transfer and document that action in the midwifery record.
If you, as the client, elect not to accept a transfer care, the midwife must terminate the midwife-client relationship. If your physician is comfortable co-managing your medical conditions while maintaining your midwife-attended delivery plan, you might not have to transfer completely. Unlike the referral conditions above, your Licensed Midwife is not allowed to continue caring for you if you refuse transfer. Transfers while you are in labor and emergency transfers are discussed more thoroughly on the TRANSFERS page.
*New as of May 2019* In years past, Texas midwives were required to refer or transfer care based on the above conditions, if they became aware. They were nothowever, required to screen you for the above conditions. As of May 2019, this screening is standard of care in any home birth midwife’s practice. She must assess at your initial visit and throughout your pregnancy for any conditions that make your pregnancy high-risk and therefore require referral or transfer.
Properly and promptly assess you when you arrive for labor and delivery. Obtain a history and perform a physical exam. Collect laboratory specimens
Monitor your progress in labor by obtaining vital signs, monitoring contractions, fetal heart tones, cervical dilation, effacement, station, presentation, membrane status, fluid intake/output, and your overall status
Assist you in the normal, spontaneous vaginal delivery of your baby
Initiate immediate emergency transfer to a hospital if she notices a dangerous condition for you or your baby. These are discussed on the TRANSFERS page.
Things your Licensed Midwife shall not do as a birth attendant in Texas:
administer any prescription drug to a client other than
a drug administered under the supervision of a licensed physician in accordance with state law (some midwives carry standing orders from a physician for drugs like pitocin to stop excessive bleeding after birth)
prophylaxis (eye ointment) approved by the Department of State Health Services to prevent ophthalmia neonatorum; or
oxygen administered in accordance with commission rule
use forceps or a surgical instrument for a procedure other than cutting the umbilical cord or providing emergency first aid during delivery (this means a non-nurse midwife may not repair any kind of vaginal or perineal laceration or “tear” with stitches)
remove placenta by invasive techniques (this means any kind of reaching inside your uterus by hand or using an instrument)
use a mechanical device or medicine to advance or retard labor or delivery (such as pitocin to augment labor or a tocolytic drug to suppress labor)
Apply fundal pressure(push on the belly toward the birth canal) during first (cervical dilation) or second (pushing) stages of labor
Administer oxytocin, ergot, or prostaglandins prior to or during first or second stage of labor. (These medications may only be used after the baby is born to control bleeding.)
make on a birth certificate a false statement or false record in violation of Section 195.003, Health and Safety Code.
Postpartum Care
The midwife must:
assess you during the immediate postpartum period by monitoring vital signs, feeling your uterus for good muscle tone, watching for bleeding, and monitoring your overall status for a minimum of two hours after your condition is stable.
Collect, assess, and document your care in the postpartum period. Develop a plan for your care and modify it as needed, and provide education and counseling to you about your condition and your baby.
Recommend referral to an appropriate professional if she notices any of the following
infection requiring antibiotics
bladder dysfunction
major depression
any other condition or symptom which could threaten your health, as assessed by a midwife exercising reasonable skill and knowledge
Initiate immediate emergency transfer and provide emergency care if she notices a dangerous condition for you or your baby. These are also discussed on the TRANSFERS page
Newborn Care During the First Six Weeks After Birth
Your midwife must provide quality care as detailed in the rules. Important things to note are that she must assess, observe and monitor your baby for at least 2 hours after delivery and recommend referral if she notices any of these conditions in the first 6 hours of life:
birth injury
gestational age assessment less than 36 weeks
small for gestational age
large for gestational age
any other abnormal newborn behavior or appearance which could adversely affect the newborn
She must also refer you to an appropriate physician if she notices any of the following after the first 6 hours of life:
abnormal lab results
minor congenital anomaly
failure to thrive
any other abnormal newborn behavior or appearance which could adversely affect the infant
She must initiate immediate emergency transfer and provide emergency care until your baby gets to a hospital if she notices any dangerous condition. These conditions are covered thoroughly on the TRANSFERS page.